Right Adrenal Mass causing Budd-Chiari Syndrome
Patient Information
Age: 5 year old
Gender: Neutered Male
Breed: English Bulldog
Weight: 74 pounds
History
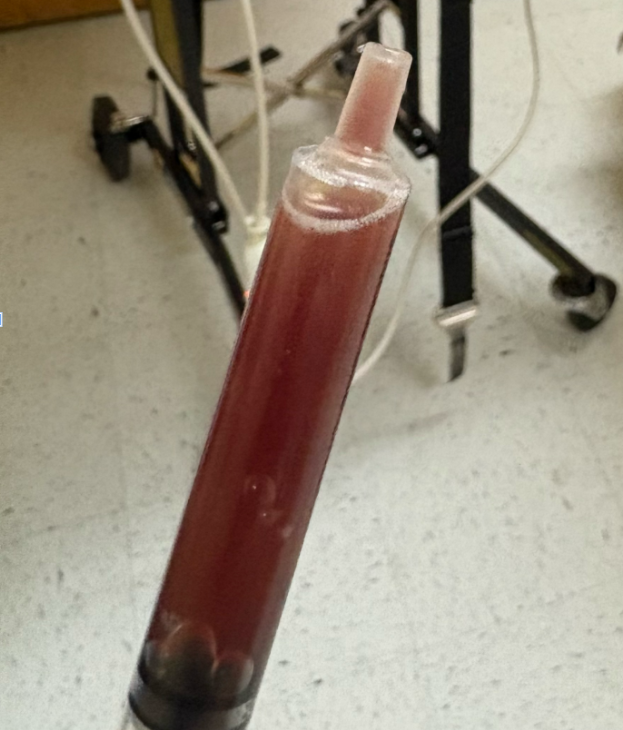
Patient was presented for polyuria and polydipsia and lethargy over a few days. Physical exam revealed a fever of 105F and a moderate volume of ascites. A diagnostic abdominocentesis revealed a thin opaque hemorrhagic fluid. Bloodwork (CBC/Chem) revealed mild eosinophilia (2.39K/uL), hyponatremia (142mmol/L) and hypochloremia (100mmol/L). The rest was within normal limits. Abdominal ultrasound was requested at this time.
Abnormal abdominal ultrasound findings -
Liver:
- Mildly enlarged and rounded in shape with coarse hypoechoic echogenicity. No focal lesions are appreciated.
Adrenal Glands:
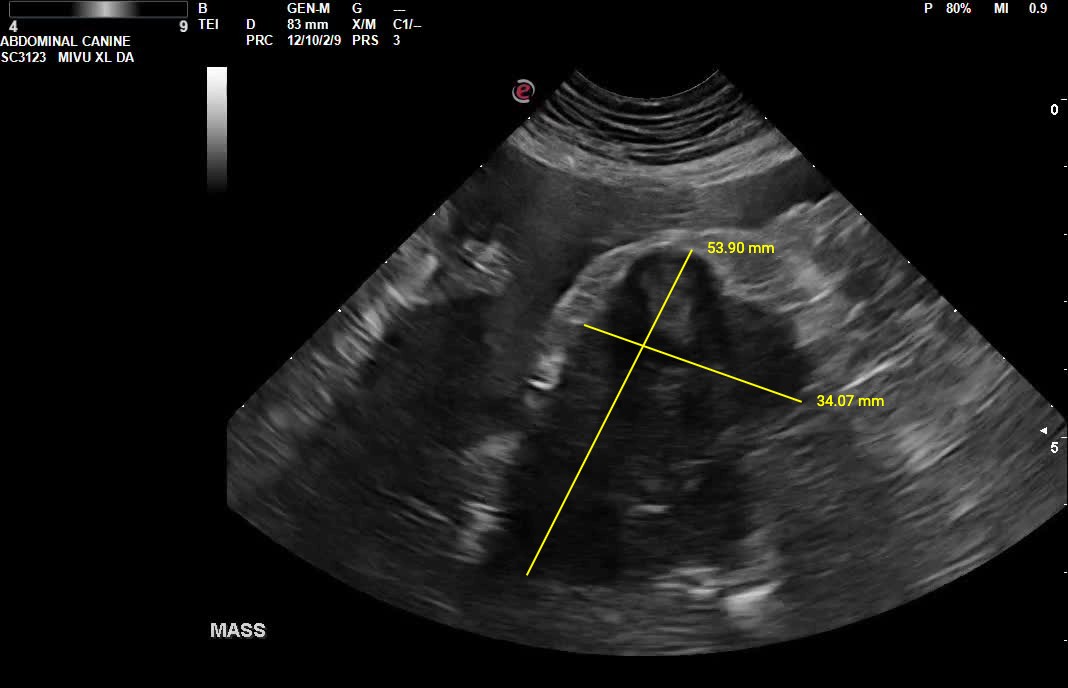
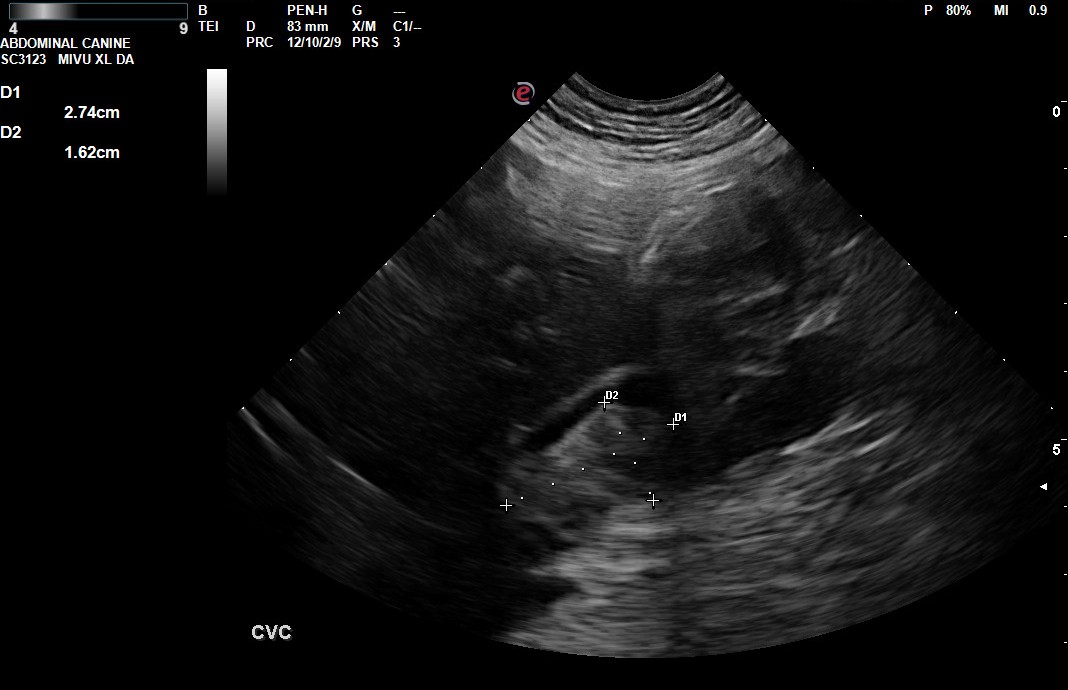
- The left adrenal gland was visualized and recognized as having normal size (Ltcd - 7.3mm) shape, size, position, and echogenicity for this breed. There is a large hypoechoic heterogenous right adrenal mass that measures 5.4x3.4cm and is compressing and invading into the caudal vena cava. There is a 2.7x1.6cm avascular structure in the caudal vena cava that is limiting blood flow.
Gastrointestinal Tract:
- The stomach is empty and collapsed with normal rugal folds and layering. The pylorus is free of obstruction. Small intestinal loops have normal bowel layering and motility. Some loops of small intestine are mildly thickened. No abnormal layering, obstruction, or masses seen. The colon has normal wall thickness and layering throughout. Duodenum 6.0mm; Jejunum 4.6-5.4mm
Serosal Surfaces/Other:
- A moderate amount of anechoic free fluid is seen throughout the abdomen.
- Mesentery throughout the abdomen is diffusely hyperechoic.
- There is a hypoechoic homogenous nodule within the mesentery in the left caudal abdomen that measures 1.9x2.0cm.
Differentials
Right Adrenal Mass - the findings are severe - DDx: differentials include cortical & medullary neoplasia vs. benign hyperplasia
- Cortical Neoplasia - Adrenal adenocarcinoma = Cushing's Dz (common)
- Non-functional adenoma vs. myelolipoma vs. hyperplasia
- Medullary Neoplasia - Pheochromocytoma (rare)
- Functional adenoma
Ascites - this finding is moderate - DDx: transudate vs. hemorrhagic vs. exudate
Liver - the findings are moderate - DDx:
- Common: Hepatitis (acute or active)
- Vacuolar hepatopathy
- Passive congestion (e.g., dilated hepatic veins and CVC)
- Cholangiohepatitis/cholangitis (acute or active)
- Neoplasia (e.g., lymphoma, sarcoma, histiocytic neoplasia, or mast cell disease)
- Less Common
- Immune-mediated hemolytic anemia
- Histoplasmosis
- Amyloidosis
- Leukemia
Intestines - the findings are mild - DDX: inflammatory bowel disease vs. food allergy/intolerance vs. infiltrative neoplasia (unlikely).
Abdominal Nodule - the findings are mild - Malignant neoplasia vs. lymph node vs. abscess vs. granuloma vs. benign neoplasm
Recommendations
- There is evidence of invasion into the caudal vena cava from the right adrenal mass as well as a thrombus in the caudal vena cava secondary to the right adrenal mass. Obstruction of blow flood is the suspected cause of the ascites (Budd-Chiari Syndrome)
- Referral for CT scan and for a surgery consultation for right adrenalectomy is recommended.
- Recommend fluid analysis of ascites.
- For intestinal changes - consider change to a novel protein diet, Texas GI panel, prophylactic deworming and fecal analysis, and/or gastrointestinal biopsies for histopathology as clinically indicated.
- Consider other diagnostics/therapeutics as clinical signs dictate.
Discussion
Large adrenal masses have the potential to invade and/or cause thrombi in the caudal vena cava which can partially or completely obstruct blood flow. In this case, the obstruction of the caudal vena cava is the suspected cause of ascites as seen in secondary Budd-Chiari syndrome. This condition is characterized by compression or invasion of the caudal vena cava from a lesion originating outside of the vasculature. Obstruction of the hepatic veins (either where they enter the caudal vena cava or cranial to the entrance of the hepatic veins) can cause venous congestion and hepatic injury. This is a life threatening condition with acute, subacute, and chronic forms. In this case, a CT scan for further characterization of the adrenal mass and its secondary effects in the vena cava were recommended to determine a surgical approach for right adrenalectomy.
Outcome
Unfortunately this patient passed away at home before it was possible to be seen by a specialist.
Citations
Mattoon, John S., Rance K. Sellon, and Clifford R. Berry, editors. Small Animal Diagnostic Ultrasound. 4th ed., St. Louis, MO: Elsevier, 2021.
Hitawala, Asif A., and Eric Goosenberg. “Budd‑Chiari Syndrome.” StatPearls, StatPearls Publishing, 6 Apr. 2025, https://www.ncbi.nlm.nih.gov/books/NBK558941/.
Special thanks to Crossroads West Veterinary Center for their collaboration on this interesting case