UTI signs lead to diagnosis of Metastatic Apocrine Gland Anal Sac Adenocarcinoma(AGASACA)
SIGNALMENT:
Breed: Heeler
Age: 10y
Sex: Spayed Female
HISTORY:
History of bilateral curiate repairs. No other significant history until she presented with signs of a suspected urinary tract infection including urinary accidents in the home.
Labwork:
Urinalysis and Chemistry were performed and revealed:
Urinalysis - 2+RBC, 1+Cocci
Chemistry- Hypercalcemia(15.7 mg/dL (reference range: 7.900-12.000)), Mild bilirubinemia(TBIL 1.3 mg/dL)
Physical Exam Findings:
A small lobulated string of masses was palpated on the left wall of the rectum associated with the anal sac.
ULTRASOUND FINDINGS:
The medial iliac lymph nodes are mild-moderately enlarged with rounded shape having heterogenous mildly hypoechoic echogenicity. Left - 2.2cm depth, 4.5cm length Rt: 1.0cm Depth
The remainder of the abdomen was found to be free of ultrasonographic lesions.
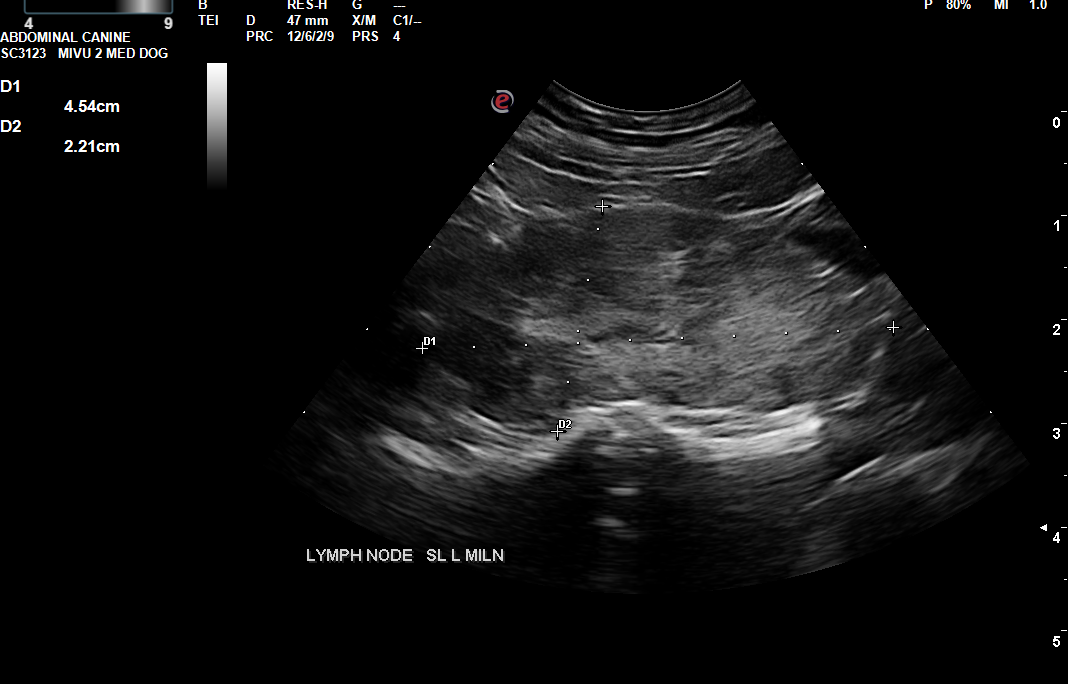
Image 1- Enlarged, rounded, hypoechoic heterogenous left medial iliac lymph node.
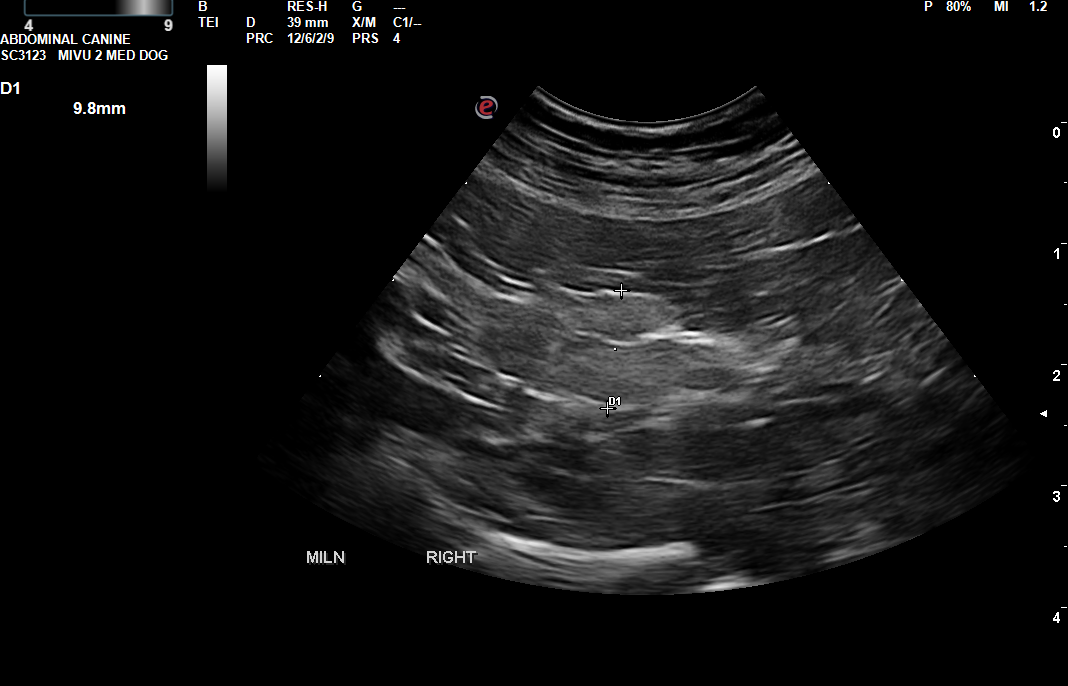
Image 2- Mildly enlarged right medial iliac lymph node.
CYTOLOGIC DIAGNOSIS AND FINDINGS:
Diagnosis
Consistent with metastatic apocrine gland adenocarcinoma of the anal sac
Comments
The diagnosis of an anal gland adenocarcinoma is suspected with 95% confidence. Other tissues that exhibit an endocrine/neuroendocrine morphology cannot be ruled out, but these other etiologies are not typically associated with hypercalcemia.
Microscopic description
The slides are lightly to moderately cellular and consist of few to many red blood cells and a nucleated cell population predominated by cells with poorly defined cell borders in loosely cohesive clusters. These cells have a lightly basophilic cytoplasm and a round to oval nucleus with loosely clumped to finely stippled chromatin and indistinct nucleoli. Anisokaryosis is minimal. Clusters are occasionally arranged in acinar structures. Few leukocytes in proportions consistent with peripheral blood are also present.
Image 3: Cytology - A nucleated cell population predominated by cells with poorly defined cell borders in loosely cohesive clusters. These cells have a lightly basophilic cytoplasm and a round to oval nucleus with loosely clumped to finely stippled chromatin and indistinct nucleoli. Anisokaryosis is minimal. Clusters are occasionally arranged in acinar structures. Few leukocytes in proportions consistent with peripheral blood are also present.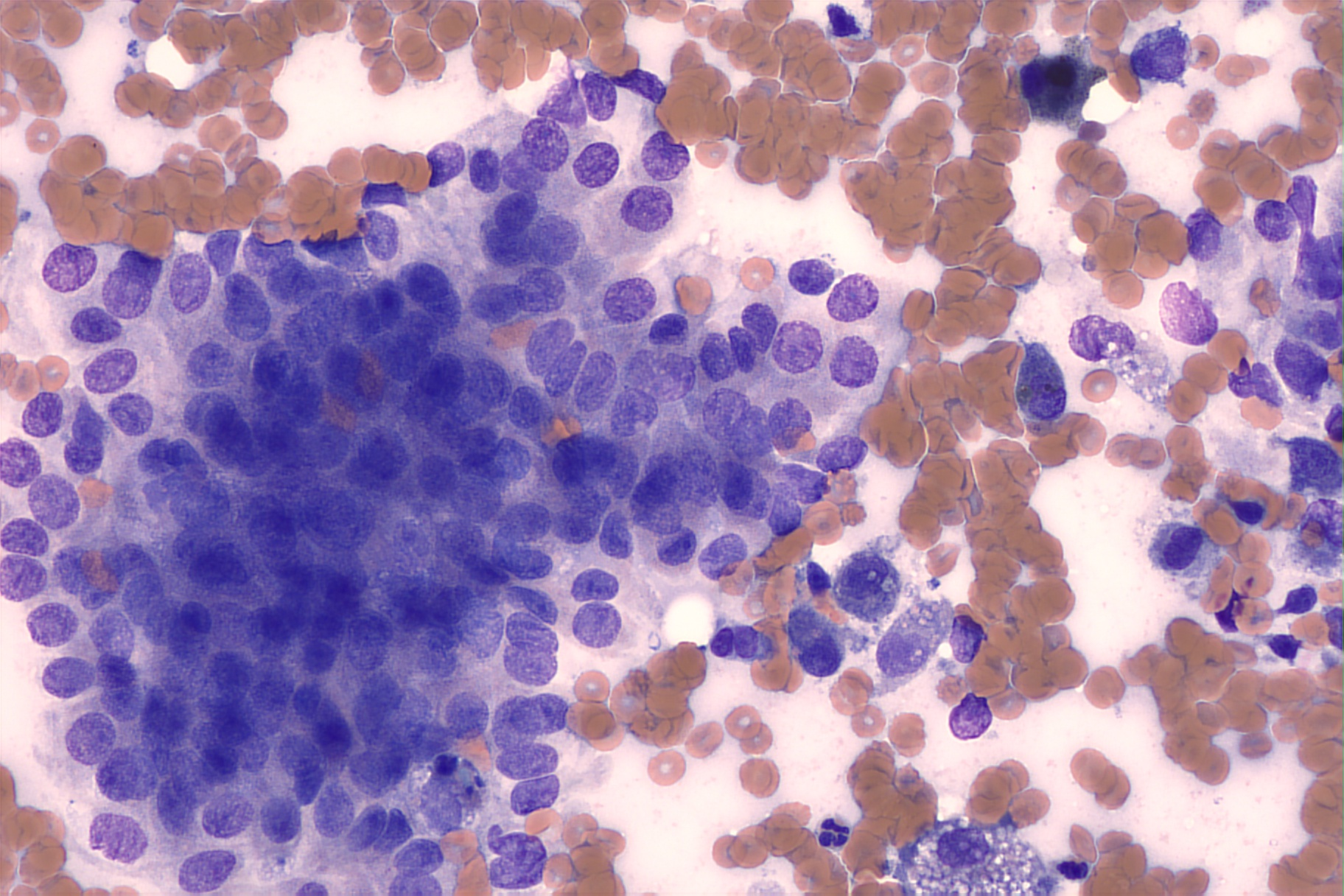
Plan:
Thoracic radiographs taken and no evidence of further metastasis were identified.
The patient was taken to a veterinary oncologist for further evaluation and best therapeutic planning.
She had surgical AGASACA and metastatic lymph node excision with a veterinary surgeon followed by six rounds of chemotherapy.
DISCUSSION:
An initial appointment for suspected urinary signs and a urinary tract infection unfortunately revealed an unexpected diagnosis of metastatic AGASACA.
A significant percentage of dogs with AGASACAs, up to 53%, show clinical signs related to paraneoplastic hypercalcemia. These signs, commonly increased urination (polyuria) and excessive thirst (polydipsia), can be easily misdiagnosed as a UTI without a comprehensive urinalysis and blood chemistry panel.
AGASACAs are known to be locally aggressive with a high rate of early metastasis. Research indicates that up to 83% may metastasize to the iliosacral lymph nodes, and emerging studies suggest a strong association with lymph node metastasis even in tumors smaller than 2.0 cm.
Prognostic indicators for AGASACA outcomes include: primary tumor size, presence of clinical symptoms, metastatic regional lymphadenopathy at initial presentation, size of metastatic lymph nodes, presence of distant metastases at diagnosis, histological characteristics of the primary tumor, and the presence of hypercalcemia.
Given the high risk of metastasis and potential for lymphadenectomy to improve outcome, abdominal ultrasound or other advanced imaging is strongly recommended before AGASACA excision.
OUTCOME: It has been over 18 months since Sasha’s initial diagnosis and we were thrilled to find out she continues to do well with no recurrence!

REFERENCES:
Jones AE, Wustefeld-Janssens BG. A relatively high proportion of dogs with small apocrine gland anal sac adenocarcinoma (AGASACA) primary tumours present with locoregional lymph node metastasis. Vet Comp Oncol. 2023 Jun;21(2):327-331. doi: 10.1111/vco.12890. Epub 2023 Mar 8. PMID: 36861227.
Repasy AB, Selmic LE, Kisseberth WC. Canine Apocrine Gland Anal Sac Adenocarcinoma: A Review. Top Companion Anim Med. 2022 Sep-Oct;50:100682. doi: 10.1016/j.tcam.2022.100682. Epub 2022 Jul 2. PMID: 35792243.
Tanis J., Simlett-Moss A.B., Ossowksa M., Maddox T.W., Guillem J., Lopez-Jimenez C., Polton G., Burrow R., Finotello R. Canine Anal Sac Gland Carcinoma with Regional Lymph Node Metastases Treated with Sacculectomy and Lymphadenectomy: Outcome and Possible Prognostic Factors. Vet. Comp. Oncol. 2022;20:276–292. doi: 10.1111/vco.12774.
Thank you to Banfield Mechanicsville and Casey Leblanc with Eastern Vetpath for collaborating with us on this case!