April's Case of the Month - 2026 brought to you by Dr. Amy Delano.
A Case of Suspected Triaditis and Pancreatoliths in a Cat
Patient information:
Age: 13 years
Gender: Neutered male
Breed: Domestic shorthair
Weight: 9.66lb
History:
The patient presented to the primary care veterinarian for acute vomiting with hematemesis and anorexia. On physical exam, he was noted to have weight loss/lean body condition (BCS 4/9) and dental tartar. Bloodwork showed elevated liver enzymes, mild hyperlipasemia, and hypochloremia. Initially, he responded well to supportive care (sucralfate, a prescription gastrointestinal diet, an oral antiemetic PRN, and clavamox), but then represented 8 days after initial presentation for ongoing anorexia and decreased defecation. The patient was started on an appetite stimulant and sent home with a highly palatable prescription diet. An abdominal ultrasound was recommended by the primary care veterinarian.
Biochemical findings:
ALT 757 High
AST 529 High
Lipase 102 High
Cl 113 Low
Otherwise unremarkable
Urinalysis:
USG 1.039
RBC >100 RBC/hpf)
WBC (6-10 WBC/hpf)
3+ protein
No bacteria, casts, or crystals
Ultrasound findings:
Kidneys - Normal size (Lt/Rt = 4.0 /3.8cm ) and shape with coarse mildly hyperechoic renal cortices and moderately reduced corticomedullary junction distinction. A scant amount of pyelectasia is seen in both kidneys (Ltpye/Rtpye = 2.0 /1.5mm ).
Pancreas - The right limb of the pancreas is normal in size (0.7cm depth with a pancreatic duct depth of 1.5mm) and overall echogenicity. There is a round, hyperechoic shadowing structure measuring 0.4cm in diameter consistent with a pancreatolith located in the pancreatic duct in the right pancreas. The left limb of the pancreas is prominent with marked dilation of the pancreatic duct (5.6mm depth). There is a mixed echogenicity structure present in the pancreatic duct in the distal aspect of the left limb of the pancreas measuring 0.9cm D x 1.9cm L. The fat surrounding the left limb of the pancreas is moderately hyperechoic.
(normal pancreatic duct diameter in cats is < 2.5mm)
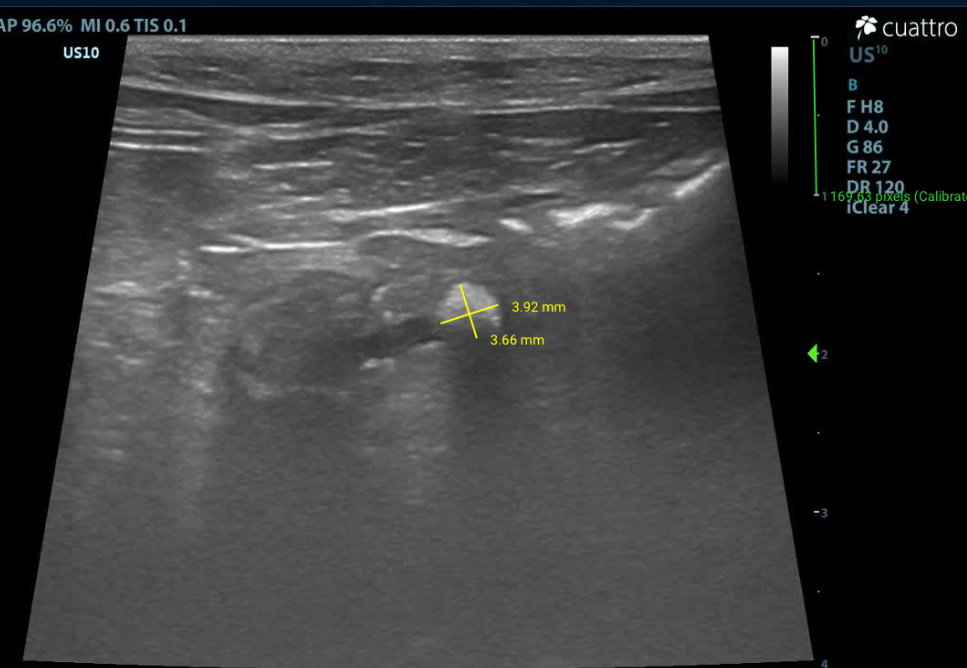
Pancreatolith in right limb of pancreas
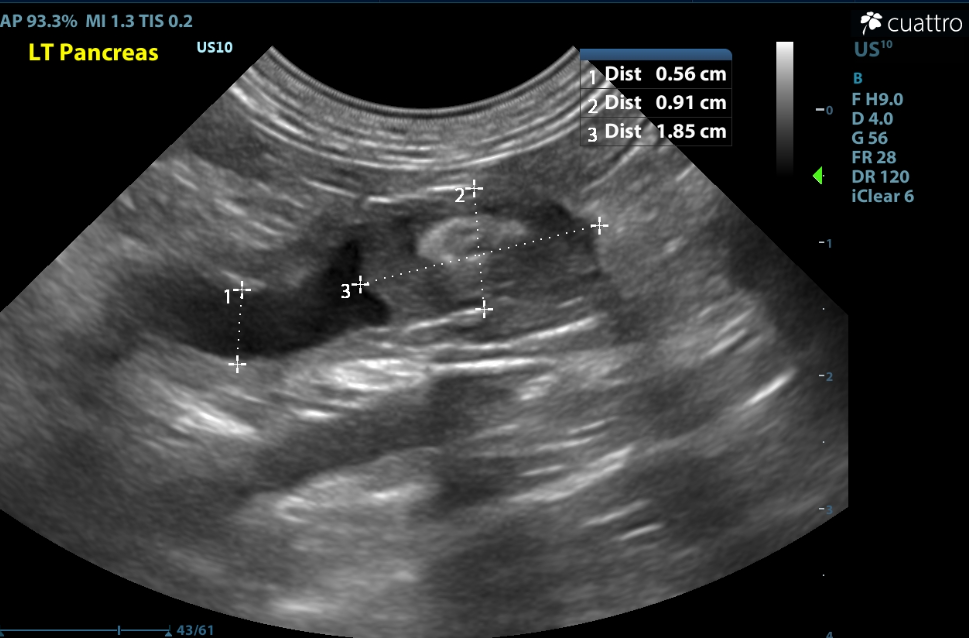
Pictured above is dilated pancreatic duct in the left limb of the pancreas with a mixed echogencity structure noted in the distal limb.
Gastrointestinal tract - The stomach contains a small amount of gas and fluid and is otherwise collapsed with normal rugal folds and layering. The pylorus is free of obstruction. Many loops of small intestine are prominent and moderately thickened measuring up to 3.4 mm (normal wall thickness ~2.2-2.5mm, > 2.8mm abnormal Norsworthy/Estep et. al. JAVMA, Vol 243, No. 10, November 15, 2013). Many have abnormal layering with splitting of the submucosal layer into 3 layers (2 hyperechoic lines split by a hypoechoic layer) and a disproportionate thickening of the muscularis layer. No obstruction or masses seen. The colon has normal wall thickness and layering throughout.
Wall thickness measurements:
Duodenum: 2.7mm
Jejunum: 2.2-3.4mm
Ileum: 3.1mm
Colon: 1.0mm
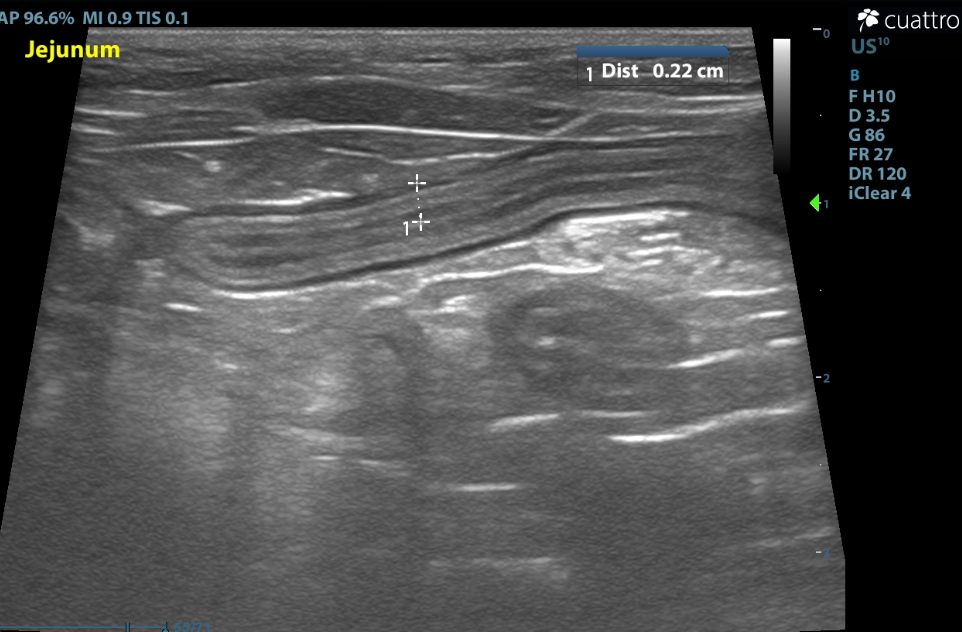
Pictured above is submucosal splitting noted in jejunum
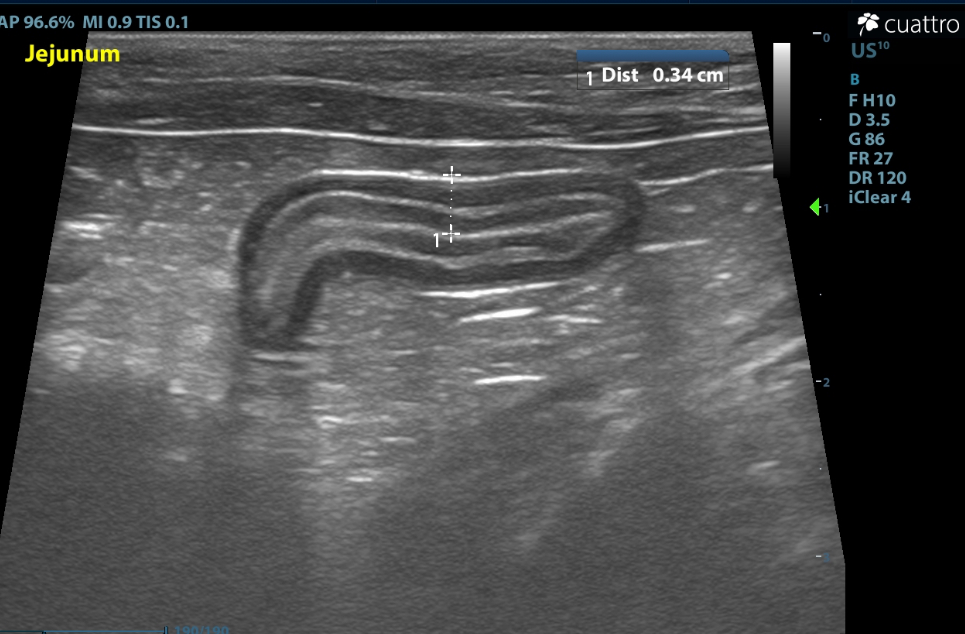
Pictured above is a moderately thickened loop of jejunum with prominent muscularis layer
Lymph nodes - A couple of mesenteric lymph nodes are mildly enlarged (measuring up to 0.6cm depth) with rounded shape having homogenous hypoechoic echogenicity.
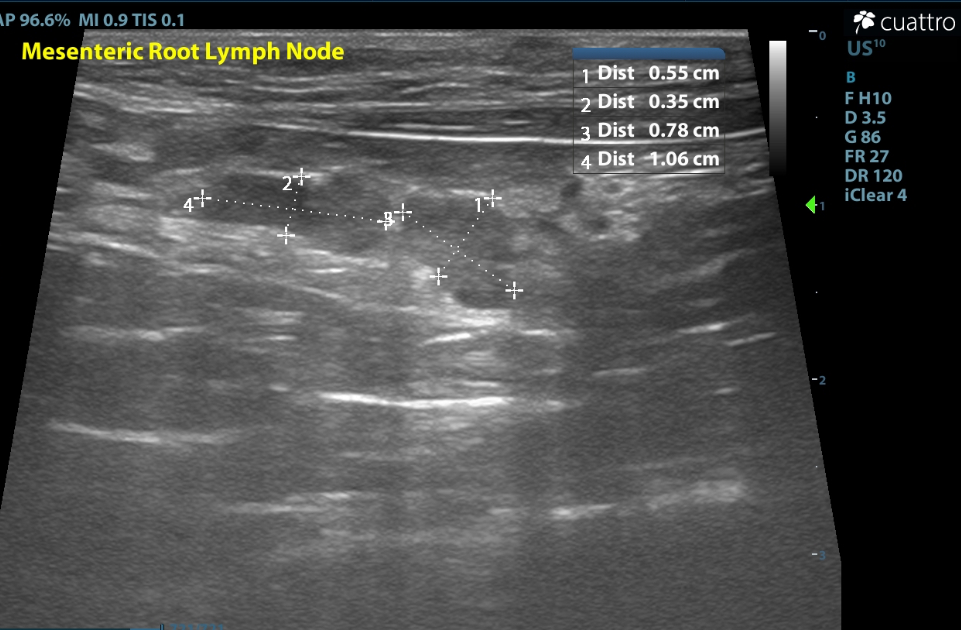
Pictured above are mildly prominent hypoechoic mesenteric lymph nodes
Differentials:
Kidneys - the findings are moderate - DDX:
a) Chronic nonspecific change - (chronic glomerulonephritis vs. amyloidosis), chronic interstitial nephritis, chronic nephritis. In cats, the loss of corticomedullary distinction is not unusual with chronic renal disease as interstitial fibrosis in the medulla renders its echogenicity similar to that of the cortex.
b) Acute renal failure/Nephritis (infectious, GN, toxic, etc.) vs. Acute-on-Chronic renal failure
c) Lymphosarcoma
d) Pyelonephritis
Intestines - the findings are moderate - DDX: mucosal fibrosis associated with inflammatory cell infiltrates vs. inflammatory bowel disease vs. infiltrative neoplasia (small-cell lymphosarcoma vs. mast cell tumor) vs. dry FIP vs. fungal (histoplasmosis). Inflammatory bowel disease in cats can be chronic and long-standing but in many cases will transition into small-cell lymphosarcoma and it is not possible with ultrasound alone to determine in this case whether the disease is benign or infiltrative.
Lymph nodes - the findings are mild - DDx: reactive vs. infection vs. IBD vs. infiltrative neoplasia (lymphoma vs. mast cell vs. other) vs. metastatic neoplasia
Feline pancreatic duct dilation - the findings are moderate - DDx: suppurative pancreatitis vs. infection/abscessation vs. age-related change
Pancreas (left limb) - the findings are moderate - DDx: pancreatolith vs. inspissated abscess vs. granuloma vs. neoplasia
Pancreas (right limb) - the findings are mild - DDx: pancreatolith
Recommendations:
- There are significant changes in the pancreas that are suggestive of pancreatitis and pancreatoliths. Pancreatolithiasis is rare in cats and has been associated with chronic pancreatitis and triaditis.
- There are diffuse changes throughout most of the small intestinal tract. Inflammatory bowel disease is favored over neoplasia, however, intestinal biopsies would be needed to definitively diagnose the pathology present.
- Standard of care for definitive diagnosis of small intestinal disease in cats is full thickness or endoscopic biopsies of the small bowel for histopathology (Ref: Norsworthy/Estep et. al. JAVMA, Vol 243, No. 10, November 15, 2013). However, for palliative empirical treatment of idiopathic inflammatory bowel disease or small cell lymphoma, if response to prednisolone is not optimal, chlorambucil can be used as an adjunctive therapy. There are several dosing protocols that have been reported. For cats that are relatively easy to pill, a dose of 2mg/cat, PO, three times a week, can be used. In smaller cats or cats that don't tolerate chlorambucil well, the dose frequency can be reduced to twice weekly. For cats that are harder to pill, pulse dosing can be used. This entails giving a dose of chlorambucil 20mg/m2, PO, once every 2 weeks. Generally this drug is very well tolerated in cats but it may cause myelosuppression so complete blood counts should be monitored periodically. Some cats with IBD or lymphoma also have comorbid conditions, such as diabetes, that mean the use of prednisolone is contraindicated. Budesonide is a corticosteroid which is extensively metabolized on its first pass through the liver. This means it causes fewer systemic side effects than prednisolone. In these cases, budesonide can be used instead of prednisolone. However, there may still be some systemic side effects associated with this drug. A dose of 1mg per cat, PO, q24 hours has been recommended. —Jonathan Lindbury, BVMS, Dip ACVIM, Dip ECVIM, MRCVS; 19th Tex A&M CVM Feline Forum, 2015.
- Consider diet change to novel protein diet or hydrolyzed protein diet.
- Consider broad spectrum prophylactic deworming and fecal analysis if not already performed.
- Consider a Texas A&M GI panel and specfPL if not already done.
- No obvious abnormalities are present in the liver; however this does not rule out disease. Pursue further diagnostics as appropriate (bile acids, biopsies, etc). In the meantime, consider hepatoprotectants.
- The changes to the kidneys are most consistent with chronic change. Continue monitoring renal parameters and consider urinalysis with urine culture and sensitivity and systemic blood pressure if not recently performed.
- The mildly enlarged mesenteric lymph nodes are likely reactive in nature.
- Consider other diagnostics/therapeutics as clinical signs dictate.
Discussion:
In human medicine, a majority of cases of chronic pancreatitis have pancreatoliths noted as a sequela. However, in veterinary medicine, pancreatolithiasis is rare in cats. As of 2021, only 5 feline cases have been reported in the literature. There is some evidence that pancreatoliths can form in cats with chronic pancreatitis with or without triaditis [1]. Stone analysis of a few cases have revealed 100% calcium carbonate composition [1], [3].
“Triaditis” is a term referring to a disease process in cats that occurs when inflammation is present in the small intestines, liver, and pancreas concomitantly. The full pathogenesis and etiology is not completely understood. Diagnosis of triaditis usually involves a combination of history, physical exam, laboratory findings, and diagnostic imaging such as ultrasound. A true definitive diagnosis is not often made as this requires histopathology [2]. Triaditis is often treated presumptively with supportive care such as anti-emetics, fluid support, nutritional support (feeding tubes vs. appetite stimulants), pain management, antibiotics, and steroid therapy. Prognosis is variable depending on the severity of the case [2].
Given the limited cases of pancreatoliths reported in the literature, treatment options for obstructive pancreatolithiasis are limited when compared to human medicine. A few cases have been treated surgically with varying degrees of success [1].
Outcome:
At the time of the ultrasound the patient had clinically improved with antibiotics and supportive care. It is suspected that this patient had an acute flare up of pancreatitis/triaditis when his illness began earlier this month given the changes in the intestines and pancreas on ultrasound and the elevated liver values in bloodwork. The pancreatoliths did not appear to be causing an obstruction. It was recommended that in the future, if this patient develops clinical signs of illness, recommend rechecking a liver panel including total bilirubin to ensure that the patient hasn’t developed an extrahepatic biliary obstruction from a choledocholith (stone in the common bile duct). It was also recommended to consider a recheck ultrasound in 2-3 months as a comparative study.
Reference:
- Frederik Allan, Ann-Lorraine Peschard, Luca Schiavo, Will Bayton, Davide Corbetta, Katie E McCallum. Obstructive pancreatolithiasis in a cat with triaditis and concurrent hypercalcaemia. JFMS Open Rep. 2021 Mar 18; 7(1): 20551169219998494.doi: 10.1177/2055116921998494
- Albert E Jergens. Feline Triaditis: Truth and Consequences. ACVC 2021.
- Annie Wayne, Pamela Mouser, Douglas Brum. Pathology in Practice. Pancreatolithiasis. J Am Vet Med Assoc. October 2013; 243(7):971-3.