May's Case of the Month 2026
Three Cases of Patent Ductus Arteriosus in Mature Dogs Ages 5-11 Years of Age
Signalments
Patient A
Age: 9 years
Gender: Intact Female
Species: Canine
Breed: Terrier Mix
Weight: 4.2 kg
Patient B
Age: 5 years
Gender: Neutered Male
Species: Canine
Breed: Yorkshire Terrier
Weight: 1.1 kg
Patient C
Age: 11 years
Gender: Neutered Male
Species: Canine
Breed: Golden Retriever
Weight: 20 kg
History
Patient A
Patient A presented for nail trim and evaluation of coughing. The patient has been exhibiting increased clinginess and unusual sleeping behavior, attempting to sleep in bed with the owner for the past two weeks. A squeaky cough followed by gagging has been noted, occasionally producing small amounts of liquid. The patient has a known grade 6/6 heart murmur with no previous cardiac workup. The patient remains playful but activity is limited due to heart condition. The patient has experienced increased panting recently. Currently only on heartworm preventative with no other medications.
Patient B
Patient B presented for a wellness examination and vaccines. Current medications include as-needed Apoquel for seasonal allergies, which has been effective for managing symptoms during high pollen periods. Up to date with heartworm prevention (ProHeart injection), and flea/tick prevention (Bravecto). Primary concerns include dental health due to poor chewing habits and seasonal allergies causing eye discharge. The patient has a known heart murmur present since birth with no previous cardiac workup.
Patient C
Patient C has had a chronic murmur since a puppy. The owner has more recently noted lethargy and an increased respiratory rate.
Echocardiogram Findings
| Patient A Mildly increased pulmonic outflow velocities (2.1 m/s) with mild pulmonic insufficiency. Main pulmonary artery and branch dilation. The PV appears normal. Moderately elevated aortic outflow velocities (3.4 m/s) consistent with increased flow with no aortic insufficiency. No pericardial or pleural effusion noted. No obvious cardiac masses. ECG The ECG attached during the echocardiogram showed a sinus arrhythmia with frequent ventricular premature complexes, mainly isolated but with periods of ventricular bigeminy. Diagnosis The cause of the murmur is a patent ductus arteriosus (PDA). This is a congenital condition where a blood vessel present in the fetus remains open after birth. When patent, this allows blood to recirculate through the lungs inappropriately and volume overloads the left heart chambers as is seen here. There is also mild MR, TR and PR, however these are clinically insignificant at this time. It is important to note that other small congenital defects may be present, and advanced imaging with a Cardiologist is recommended. Given severe LA/LV dilation, this patient is at risk for progression to congestive heart failure, arrhythmias, PDA reversal due to development of pulmonary hypertension, exertional syncope, and/or sudden death in the future. Monitor sleeping respiratory rates at home to screen for progression to CHF. Treatment Gold standard therapy is closure of the vessel. This can be done interventionally using catheters or surgically through a thoracotomy, and consultation with a local Cardiologist is strongly recommended. Success rates for both procedures are generally high (over 95%), and a good chance for a relatively normal life, given the marked structural changes if closed appropriately. Regardless of whether or not closure is pursued, cardiac support with pimobendan benazepril and spironolactone is recommended for long term benefit. If closure is not an option, prognosis is guarded to poor long term and close monitoring is advised. Diagnosis of heart failure is based on clinical signs of increased resting respiratory rates and radiographic appearance of pulmonary edema with a positive response to furosemide. Omega fatty acid supplementation and mild salt restriction may be of some long term benefit. Monitoring of sleeping breathing rates is recommended as the best way to screen for progression to CHF at home. Mild activity restriction is advised. Monitor at home for breathing changes, worsening cough, fainting episodes, exertional dyspnea. Commence: ● Pimobendan 0.2 – 0.3 mg/kg PO q12h ● Benazepril 0.5 mg/kg PO q12h ● Spironolactone 1 – 2 mg/kg PO q12h. ● If in heart failure, furosemide 1 – 2 mg/kg every 12 hours
Simon Swift, MA, VetMB, CertSAC, DipECVIM-CA (Cardiology), MRCVS |
|
93 M-mode, color flow and Doppler images are available for review. Continuous flow detected with color Doppler in the pulmonary artery in the region of the ductus arteriosus. A PDA can be visualized which does not seem to narrow towards the pulmonary artery. High velocity shunt primarily left to right (max 6 m/s). Severe volume overload of the left heart (LV diastolic diameter 3.1, normal under 1.7; 40.8 mm) with low normal systolic function (fractional shortening 26%, normal over 25%). Increased LV sphericity. Moderate LA dilation (LA:Ao 1.74, normal under 1.6; long axis 32.1 mm). Mild central mitral regurgitation due to stretching of the mitral annulus but no obvious tricuspid regurgitation. The right heart appears normal. Normal pulmonic outflow velocities with mild pulmonic insufficiency. Main pulmonary artery and branch dilation. The PV appears normal. Moderately elevated aortic outflow velocities (3.9 m/s) consistent with increased flow with trace aortic insufficiency. No pericardial or pleural effusion noted. No obvious cardiac masses.
The ECG attached during the echocardiogram showed a normal sinus arrhythmia.
The cause of the murmur is a patent ductus arteriosus (PDA). This is a congenital condition where a blood vessel present in the fetus remains open after birth. When patent, this allows blood to recirculate through the lungs inappropriately and volume overloads the left heart chambers as is seen here. There is also trivial MR and AI, however these are clinically insignificant at this time. It is important to note that other small congenital defects may be present, and advanced imaging with a Cardiologist is recommended. Given severe LA/LV dilation, this patient is at risk for progression to congestive heart failure, arrhythmias, PDA reversal due to development of pulmonary hypertension, exertional syncope, and/or sudden death in the future. Monitor sleeping respiratory rates at home to screen for progression to CHF. Omega fatty acid supplementation and mild salt restriction may be of some long term benefit. Monitoring of sleeping breathing rates is recommended as the best way to screen for progression to CHF at home. Mild activity restriction is advised. Monitor at home for breathing changes, worsening cough, fainting episodes, exertional dyspnea. Commence: ● Pimobendan 0.2 – 0.3 mg/kg PO q12h ● Benazepril 0.5 mg/kg PO q12h ● Spironolactone 1 – 2 mg/kg PO q12h. Recommend referral to a Cardiologist. If not an option, reassess structure and function every 6 months lifelong to assess need for additional medications, sooner if clinical signs arise (progressive cough, labored breathing, syncope). Simon Swift, MA, VetMB, CertSAC, DipECVIM-CA (Cardiology), MRCVS
|
| Patient C Echocardiogram 82 2D, M-mode, color flow and Doppler images are available for review. Slightly thickened the mitral valve leaflets, moderate to severe mitral regurgitation. The left atrium measures markedly enlarged (LA:Ao 2.5, normal under 1.6; long axis [4 chamber view] 65.6 mm, normal 27.7-41.5 mm). The measured MR velocity is normal (5.5 m/s). The left ventricle (LV) measures enlarged (normalized LV diastolic diameter 2.48, normal under 1.7; 59.9 mm, normal 31-43 mm) with subjectively reduced myocardial function. The fractional shortening was 31% (normal over 25%). The mitral inflow E waves are markedly elevated at 1.7 m/s (normal < 1m/s), consistent with increased LV filling pressures. A waves are absent due to the presence of atrial fibrillation.
Moderate tricuspid regurgitation (TR) was observed. The TR velocity measured slightly elevated (3.26 m/s, normal < 2.8 m/s), most likely secondary to left sided congestive heart failure. The pulmonic and aortic valves appear normal in morphology and mobility. Normal pulmonic velocities; aortic outflow velocities upper end of normal (2 m/s, normal < 1.8 m/s). Laminar flow was present for pulmonic and aortic flow. Suspect mild aortic insufficiency; mild pulmonic insufficiency. Continuous turbulent flow in the pulmonary artery towards the pulmonic valve with adequate velocities (5.1 m/s). No pericardial or pleural effusion noted. Ascites is present. No obvious cardiac masses. ECG The ECG attached during the echocardiogram showed atrial fibrillation with a heart rate of 200-240 complexes per minute. Diagnosis Left right shunting patent ductus arteriosus (PDA), secondary left sided volume overload that has caused marked LA and LV enlargement, biventricular heart failure and atrial fibrillation. The dog is currently in biventricular heart failure and the atrial fibrillation is not controlled. Strongly recommend initiating treatment. Medications ● Pimobendan 0.3 mg/kg PO every 12 hours ● Furosemide 2 mg/kg PO every 6-8 hours initially. Depending on response to treatment (improvement of cough, reduction of resting/sleeping respiration rate) decrease to three times daily once the heart failure is well controlled (usually 3-4 days). ● Diltiazem 2 mg/kg PO three times daily (if short acting formulation). If intermediate or slow release: take the daily dose of the short acting formulation for the dog and divide into 2 doses.
● Spironolactone 2 mg/kg PO every 24 hours ● Enalapril 0.5 mg/kg PO every 12 hours
Monitor sleeping respiratory rates at home to assess response to treatment; and if control of the heart failure can be achieved, for potential decompensation in the future. Recommend re-assessment end of this week to assess response to treatment, including assessment of the heart rate (should be < 160/min) and POCUS to assess the ascites. Depending on how the dog is doing, potentially repeat thoracic radiographs. If there is no marked improvement, adjustment of medication (potentially increase of furosemide, adjustment of the treatment of the atrial fibrillation) might be required. Assess renal values and electrolytes in 7-10 days, then every 3 months while on diuretics, and after an increase in diuretics, or if inappetence and reduced water intake is present. If it is possible to stabilize patient C’s cardiac disease, a recheck ECG and possible holter monitor (24 h ECG), POCUS, echocardiogram +/- thoracic radiographs is recommended in 2-3 months, sooner if any development of associated clinical signs occurs in the interim.
Sonja Fonfara, DVM, Dr med vet, PhD, Docent, PGCertHE, CertVC, DipECVIM-CA (Cardiology)
|
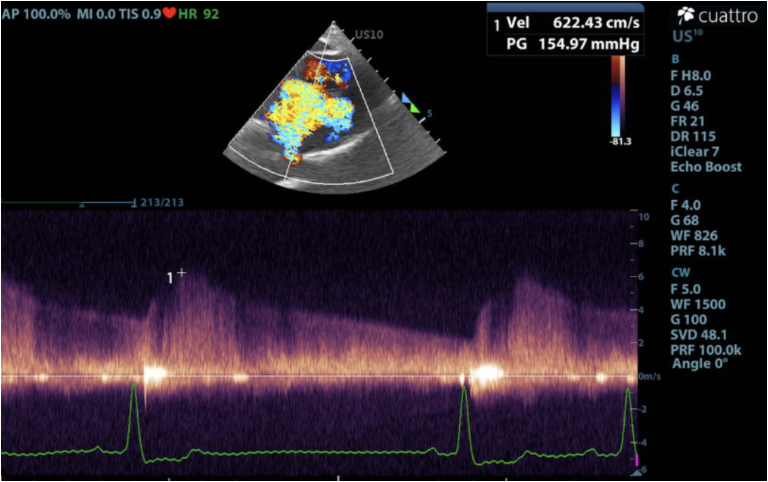
Image 1:
Continuous wave doppler showing continuous left to right flow through the PDA.
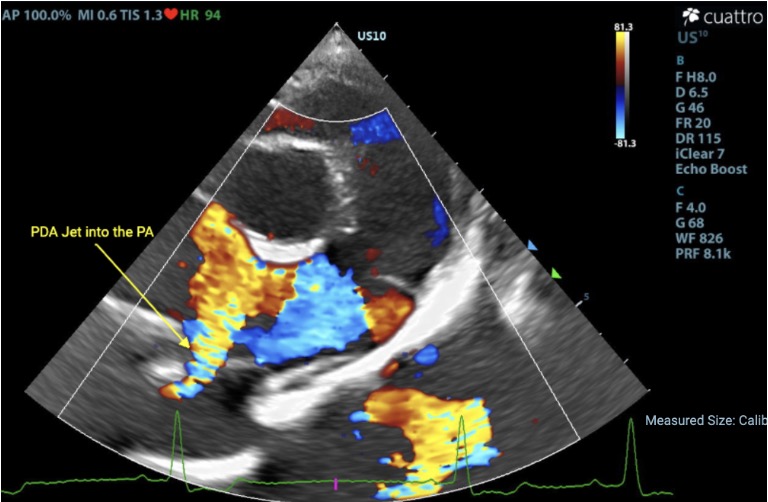
Image 2: Colorflow image within the right parasternal short axis heart base view, showing left to right shunting into the pulmonary artery.
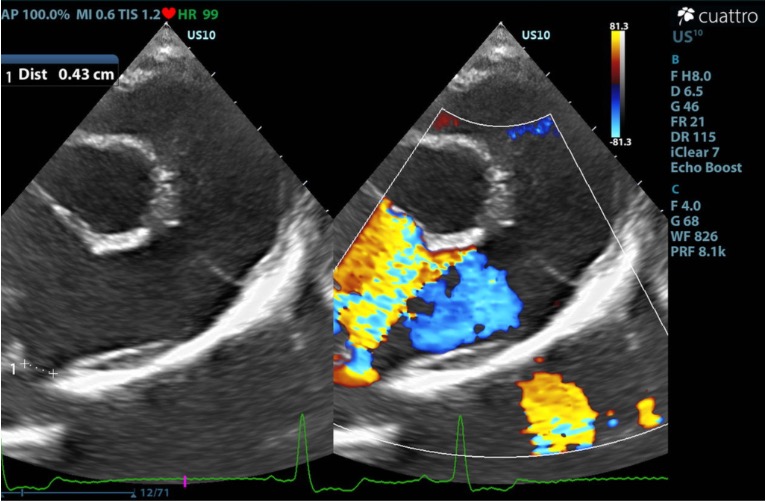
Image 3:
Colorflow image within the right parasternal short axis heart base view, showing left to right shunting into the pulmonary artery (right) with a B-mode image measuring the PDA diameter (left).
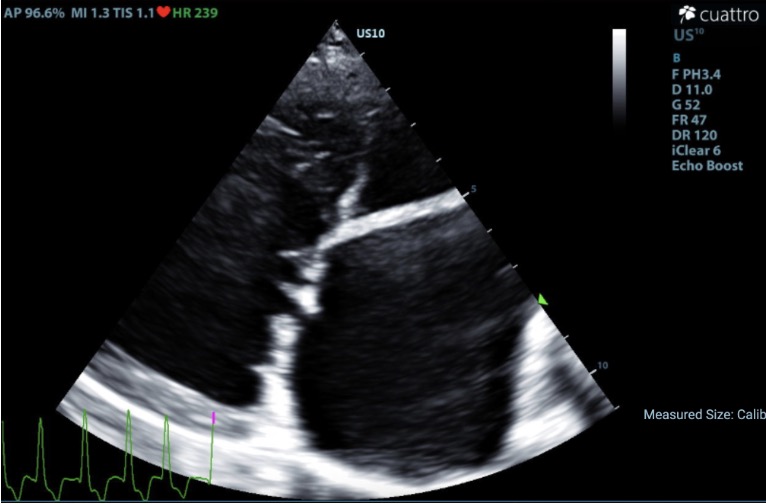
Image 4:
Right parasternal four chamber long axis view highlighting significant left atrial and left ventricular enlargement secondary to prolonged volume overload.
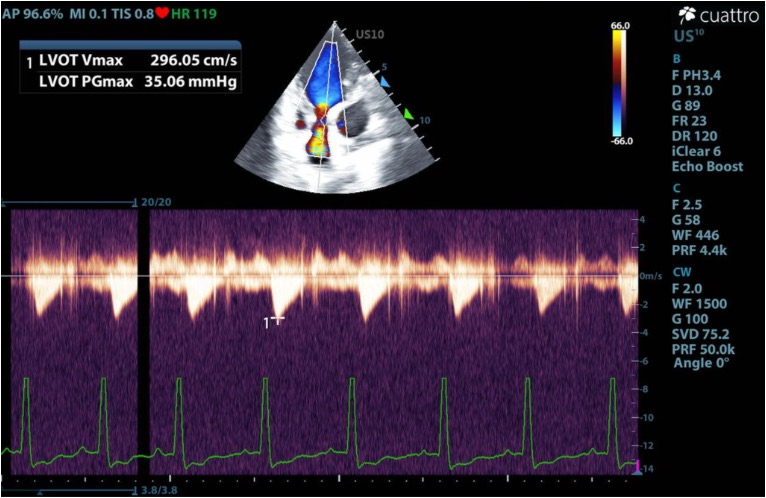
Image 5:
Continuous wave doppler in the subxiphoid view demonstrating elevated LVOT velocities. This is a common finding in patients with PDAs due to the increased stroke volume.
Outcome/Further testing:
Patient B
Patient B was referred to an interventional cardiologist, where his PDA was successfully occluded using an Amplatzer Vascular Plug 4 (AVP-4) via a minimally invasive transvascular technique. This allowed for effective closure without the need for open surgical ligation.
Repeat echocardiography performed 3 months after closure showed no residual flow through the PDA, along with significant reverse remodeling. Patient B’s clinical improvement mirrored these echocardiographic changes, with reportedly improved energy levels and resolution of his cough.
Encouragingly, given these changes, Patient B’s was able to discontinue Pimobendan and Spironolactone.
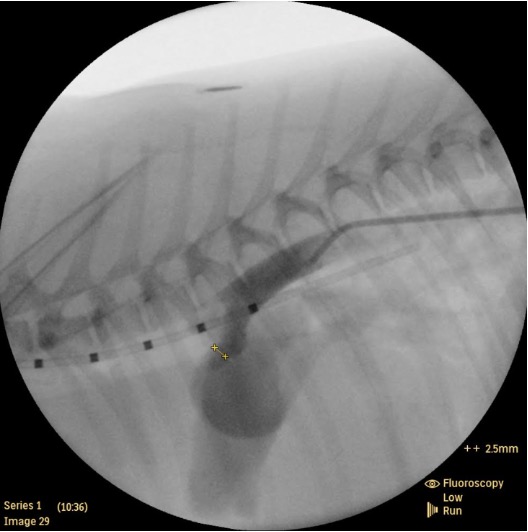
Image 1: Angiocardiogram measuring the PDA for surgical planning.
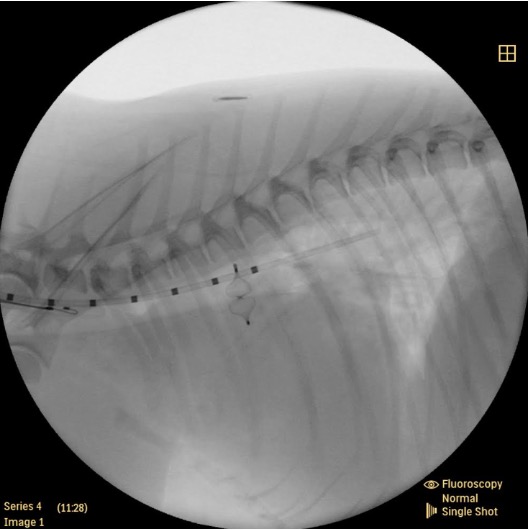
Image 2: Intraoperative image showing placement of the Amplatzer Vascular Plug 4 (AVP-4) occluder device within the PDA.
Patient A
Closure of the PDA was not pursued in Patient A’s case, and the owner instead elected to continue medical management (Furosemide, Benazopril, Spironolactone, and Pimobendan). Unfortunately, after 7 months, she was humanely euthanized after re-entering congestive heart failure.
Patient C
Patient C was very recently diagnosed with his PDA. Medical management is being pursued while the owners decide on additional intervention. The owners report clinical improvement since starting the medications.
Discussion
Understanding Physiology
In utero, oxygenated blood is delivered to the fetus through the placenta. As a result, relatively little blood is directed through the fetal pulmonary circulation. The ductus arteriosus (DA) is a normal fetal bypass vessel that allows blood leaving the right ventricle to largely bypass the lungs, diverting from the pulmonary artery into the systemic circulation. This pattern of flow, and its spontaneous transition to normal postnatal flow after birth, is governed largely by the relationship between pressure gradients and vascular resistance.
Flow (Q) = Pressure Gradient (ΔP) / Resistance (R)
In other words, blood flows down a pressure gradient, and the amount of flow through a given pathway depends, in part, on the resistance within that pathway.
In utero, blood leaves the right ventricle and enters the main pulmonary artery. There, the blood can enter the DA as well as the left and right main pulmonary arteries. In utero, pulmonary vascular resistance is high, as the lungs are not expanded and oxygen tension is low. Paradoxical to systemic circulation, pulmonary vessels constrict in response to low oxygen levels. This is the same postnatal signaling pathway which allows for preferential blood flow reaching the most well oxygenated alveoli (V/Q matching). Because the fetal lungs represent a high-resistance vascular bed, relatively little blood enters the pulmonary arteries. Instead, the DA provides a lower-resistance pathway, allowing the majority of right ventricular output to be shunted from the main pulmonary artery through the DA and back into systemic circulation. See below illustration.
Post-parturition, these same fluid dynamics reverse. With the first few breaths, oxygen tension rises within the neonatal lungs allowing for increased flow through the pulmonary circulation. At the same time, the systemic pressures rise mainly due to the loss of the placental circulation. These changes, along with many other factors beyond the scope of this discussion, allow for the transition to the normal blood flow pattern we see in our patients. Over a relatively short period of time, the DA collapses and undergoes fibrosis, transforming into the ligamentum arteriosum.
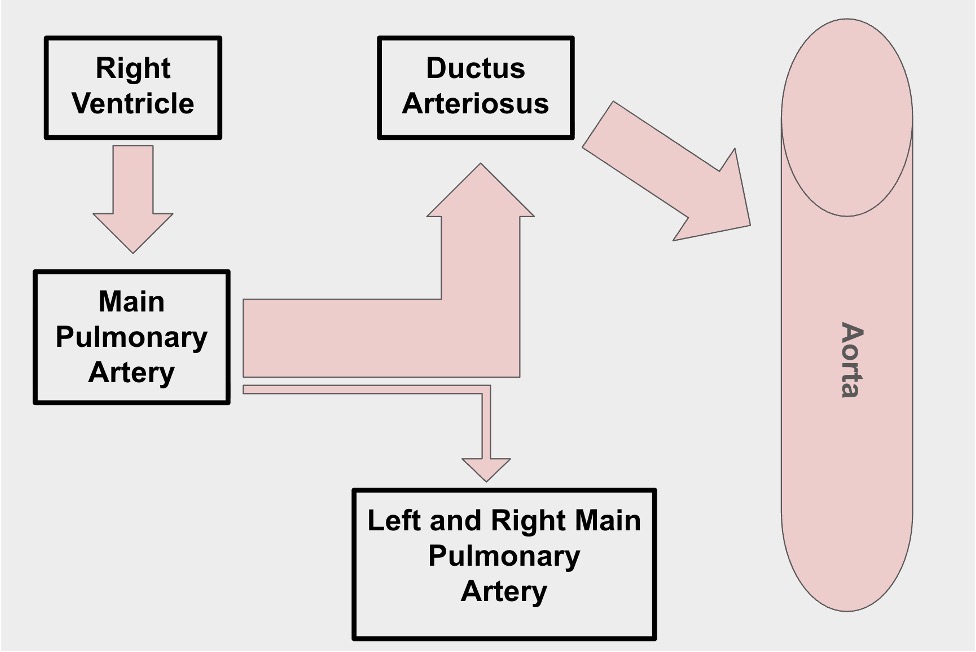
Normal fetal blood flow: Blood leaves the right ventricle, into the main pulmonary artery where the majority of flow is diverted through the DA into systemic circulation. A small amount of blood still travels through pulmonary circulation. In utero, the left atrium receives that small amount of blood from the pulmonary venous return, however, the majority of flow is received from the right atrium through the foramen ovale (not pictured in this illustration).
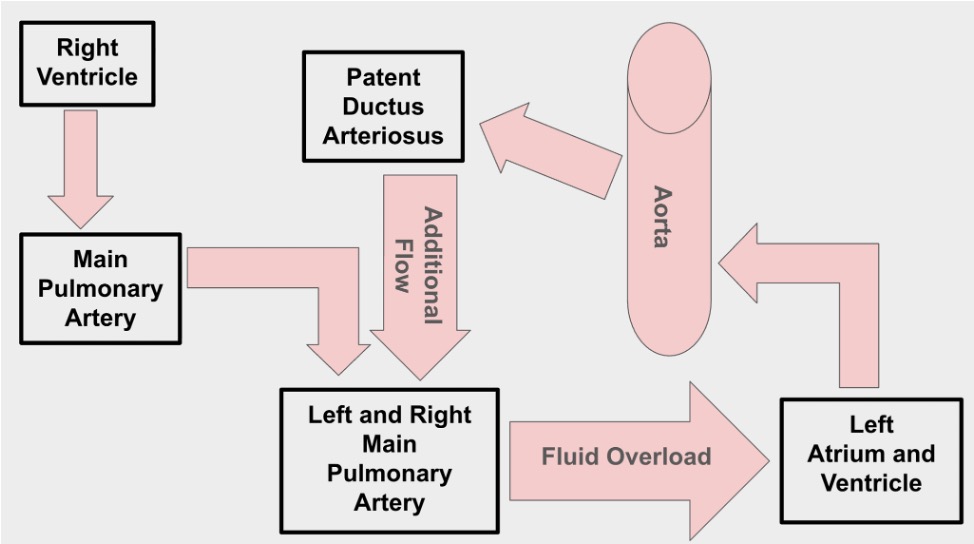
Patent ductus arteriosus blood flow: Blood from both the right ventricle and the PDA, enters into the main pulmonary artery where it is recirculated through the pulmonary vasculature and back into the left atrium and left ventricle. Over time, this additional blood being recirculated causes fluid overload of the left heart resulting in compensatory dilation and eventual decompensation.
Genetic and Histologic Changes of PDAs
In patients with patent ductus arteriosus (PDA), heritable genetic defects cause abnormalities within the wall of the ductus arteriosus. Histology of the PDA walls show variable degrees of asymmetric regions with changes in the components of smooth muscle and elastic tissue/fibers similar to what is seen within the aortic wall. [1,2] These structural abnormalities reduce the ability of the ductus arteriosus to undergo normal postnatal contraction and closure, ultimately allowing for persistent ductal patency after birth.
Importantly, this does not appear to be a simple all-or-nothing inherited defect. Rather, there is a spectrum of inherited risk, which parallels the spectrum of histologic and phenotypic changes seen within the ductus itself. As a result, patients with a lesser degree of inherited defective genome may have a relatively mild phenotypic expression, resulting in a small residual patent ductus or even a blind ductal diverticulum, which could remain asymptomatic for life.
This spectrum of genetic and histologic expression may explain why some mature patients, such as those described in these three cases, can remain relatively asymptomatic for prolonged periods, while others develop clinically significant left-sided volume overload and congestive heart failure early in life.
Treatment
As described above, PDAs generally shunt blood from the left heart (descending aorta) to the right heart, and back to the left heart. This causes an increase in blood to the left heart which eventually results in left sided volume overload and left sided congestive heart failure. As such, patients with PDAs which have progressed into congestive heart failure are treated with conventional medical therapy (diuretics, inotropes, ace inhibitors, etc.) as indicated, until further intervention can be pursued.
Historically, PDAs have been managed surgically; however, access to more advanced, minimally invasive techniques has become more widely available and utilized. This is highlighted in Benjamin’s case, where an occluding device called an Amplatzer Vascular Plug 4 (AVP-4) was delivered transvascularly through a guided catheter. These minimally invasive techniques provide several advantages over conventional surgical ligation, with improved patient comfort, decreased hospitalization time, and reduced postoperative monitoring.
Reported success rates vary. Older studies have cited successful closure rates of approximately 90% for transvascular techniques compared with approximately 98% for surgical closure. [2] However, more recent retrospective studies have reported successful closure rates of approximately 92% for transvascular occluding devices overall, and as high as 98% in cases using the Amplatz canine duct occluder (ACDO). [3] Thoracoscopic PDA occlusion has also been described [4], though it is less commonly utilized.
Overall, morbidity and mortality rates generally favor minimally invasive ductal occluder devices when compared with surgical ligation. Some studies report a 0% mortality rate for ductal occluder devices compared with approximately 2% for surgical ligation. [5] Surgical mortality rates appear dependent on surgical experience, with reported rates ranging from less than 2% to as high as 8%. [2] Morbidity follows a similar pattern, with minimally invasive ductal occlusion generally associated with fewer complications than conventional surgical ligation.
The age at presentation/closure of PDAs has been shown to be an important factor in long-term reverse remodeling in dogs. [6] Fortunately for Patient B, significant reverse remodeling to near normal cardiac dimensions has been noted in the most recent follow up. This same remodeling capacity would likely be diminished in Patient A and Patient C’s cases given their age (among other factors).
It is important to note that not all patients are optimal candidates for minimally invasive techniques, and further assessment with an interventional cardiologist is necessary to evaluate factors such as patient size, PDA diameter, and PDA type/morphology before determining the optimal treatment plan. Furthermore, some patients with a chronic PDA may also develop significant pulmonary hypertension to the point that ductal flow becomes bidirectional or reverses right-to-left, creating an Eisenmenger-like syndrome. In these severe cases, closure of the PDA is generally contraindicated as closure would redirect flow back through the pulmonary vasculature and worsen the already severe pulmonary hypertension.
Early recognition and intervention can provide substantial benefit to our patients’ long term prognosis and quality of life. These cases demonstrate the importance of early echocardiography within the field.
References
- Buchanan JW, Patterson DF. Etiology of patent ductus arteriosus in dogs. J Vet Intern Med. 2003 Mar-Apr;17(2):167-71. doi: 10.1111/j.1939-1676.2003.tb02429.x. PMID: 12683616.
- Broaddus KD, Tillson DM. “Patent Ductus Arteriosus in Dogs.” Compendium. 2010.
- M. K. Singh, M. D. Kittleson, P. H. Kass, L. G. Griffiths, Occlusion Devices and Approaches in Canine Patent Ductus Arteriosus: Comparison of Outcomes, Journal of Veterinary Internal Medicine, Volume 26, Issue 1, January-February 2012, Pages 85–92, https://doi.org/10.1111/j.1939-1676.2011.00859.x
- Borenstein N, Behr L, Chetboul V, Tessier D, Nicole A, Jacquet J, Carlos C, Retortillo J, Fayolle P, Pouchelon JL, Daniel P, Laborde F. Minimally invasive patent ductus arteriosus occlusion in 5 dogs. Vet Surg. 2004 Jul-Aug;33(4):309-13. doi: 10.1111/j.1532-950X.2004.04045.x. PMID: 15230832.
- Ranganathan B, LeBlanc NL, Scollan KF, Townsend KL, Agarwal D, Milovancev M. Comparison of major complication and survival rates between surgical ligation and use of a canine ductal occluder device for treatment of dogs with left-to-right shunting patent ductus arteriosus. J Am Vet Med Assoc. 2018 Oct 15;253(8):1046-1052. doi: 10.2460/javma.253.8.1046. PMID: 30272512.
- Saunders AB, Gordon SG, Boggess MM, Miller MW. Long-term outcome in dogs with patent ductus arteriosus: 520 cases (1994-2009). J Vet Intern Med. 2014 Mar-Apr;28(2):401-10. doi: 10.1111/jvim.12267. Epub 2013 Dec 26. PMID: 24372855; PMCID: PMC4857963.