Incidental Renal Tumor in Dog with suspected Pituitary-dependent hyperadrenocorticism (PDH)
Patient Information:
Age: 11 years
Gender: Spayed Female
Breed: Pomeranian Mix
HISTORY:
The patient presented for a routine annual exam and full senior blood work. The patient has a history of hypothyroidism and is currently well regulated. . The thyroid value came back within range but the patient's liver values had increased since previous blood work was done (~ October 31, 2024). The patient is mildly overweight and had dental calculus with no other clinically significant exam findings.
BIOCHEMICAL ABNORMALITIES:
Historically 2024
ALT 193 U/L
ALKP 354 U/L
Currently
ALT 412 U/L
ALKP 1057 U/L
GGT 16 U/L
ULTRASOUND FINDINGS:
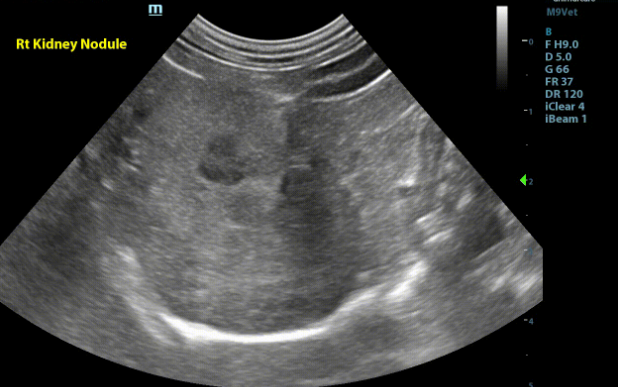
Kidneys - Both kidneys were found to have normal size (Lt/Rt = 3.8 /4.0cm). With a normal overall shape with coarse mild to moderately hyperechoic renal cortices which are mildly enlarged. There was mild loss of the corticomedullary junction distinction. There were a few small thin-walled anechoic cortical cysts seen throughout both kidneys. There is a homogenous, well defined, hypoechoic very mildly capsule deforming nodule affecting the corticomedullary region in the convex portion of the right kidney. (1.1x0.8cm)
No pyelectasia was seen.
Liver - The liver was mild-moderately increased in size, mildly rounded shape and moderately coarse hyperechoic echogenicity. No focal lesions are appreciated. The gallbladder was moderately enlarged and rounded in shape having hyperechoic mildly organizing bile sludge with subtle radiating linear striations along the periphery consistent with an emerging gallbladder mucocele.
Adrenals - Both adrenal glands were visualized and recognized as having abnormally rounded "plump" shape, increased size (Lt/Rt = 6.5/5.9 mm), normal position with stimulated overall echogenicity for this breed. No adrenal invasion into the vena cava, phrenic vein thrombosis, dystrophic mineralization or clinically significant nodular changes were noted.
Pancreas - The pancreas was increased in size, plump shape, coarse mildly hypoechoic echogenicity. No focal lesions seen. Peripancreatic fat was normal in echogenicity.
Gastrointestinal System - The stomach was empty and collapsed with normal rugal folds and layering. The pylorus is free of obstruction. Small intestinal loops have normal bowel layering, thickness, and motility. Duodenum 5.5mm, Jejunum 2.4-3.7mm No abnormal layering, obstruction, or masses seen. The colon had normal to mildly increased wall thickness and normal layering throughout.(2.4-3.6mm)
Spleen - The spleen was a normal size(1.2cm), shape, and echogenicity. There was a small homogenous, irregular nodular projection from the tail of the spleen. (0.9x0.7cm)
Image 1 - Right kidney in sagittal with small hypoechoic well defined nodule
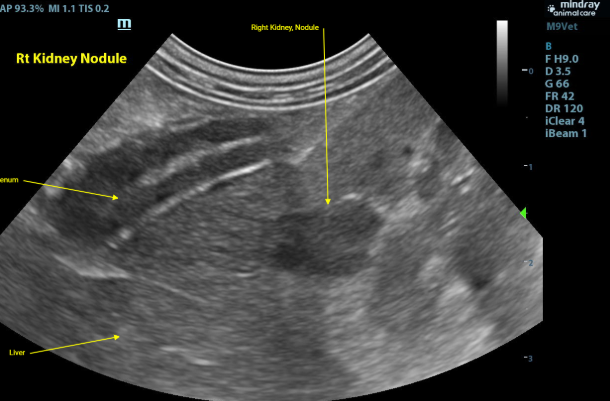
Image 2: Right kidney in transverse with hypoechoic nodule
FURTHER INVESTIGATION:
Ultrasound guided fine needle biopsies of the right renal nodule were collected and submitted for cytology.
CYTOLOGIC DIAGNOSIS AND FINDINGS:
The cytologic findings are consistent with epithelial cell proliferation. Given the lack of atypia a benign process (adenoma) is not excluded. A well differentiated carcinoma is also a differential.
Image 3: Cytology
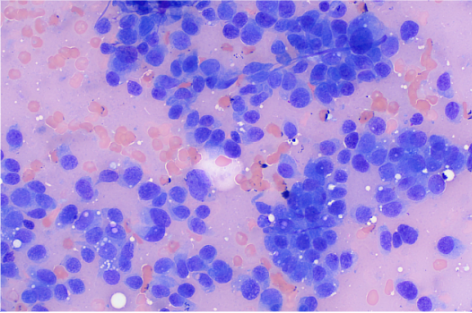
Image 4: Cytology
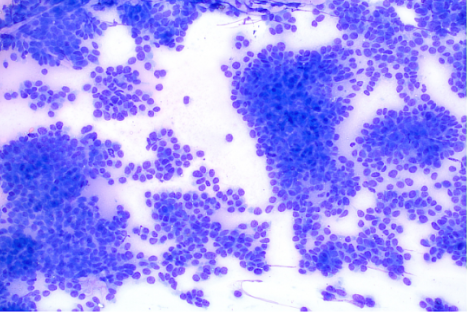
The sample is of moderate cellularity and adequate preservation. Aggregates of atypical cohesive cells are present on an eosinophilic background with erythrocytes. The cohesive cells are seen in papillary-like formations. These rounded to sometimes fusiform cells have distinct cellular borders with a small amount of pale to medium basophilic cytoplasm, occasionally with clear round vacuoles. The round to oval nuclei measure approximately 1-2 times the diameter of erythrocyte with coarsely stippled chromatin, containing 1-2 small distinct nucleoli. Anisocytosis and anisokaryosis are mild with a high nucleus to cytoplasm ratio. Neutrophils are rarely found on scanning, likely in accord with the degree of hemodilution. Rare glomerular tufts are seen on scanning. No infectious agents are identified.
DISCUSSION:
In dogs, most renal tumors (~70%) originate from epithelial cells, with 25% derived from mesenchymal cells, and the remaining 5% being nephroblastomas. The most common epithelial lesions are renal carcinomas, followed by rare and benign renal adenomas and oncocytomas, as well as transitional cell papillomas and carcinomas. Definitive diagnosis requires a biopsy for histopathology.
The metastatic rate for renal carcinomas is reported to be between 50% and 60%. Renal neoplasia commonly metastasizes to the lungs, lymph nodes, liver, and adrenal gland The lesion found in this patient's kidney was small at the time of sampling and lacked signs of cellular atypia, suggesting it may be an incidental, benign adenoma. The remaining changes in the abdomen of this patient were mostly consistent with age related or pituitary-dependent hyperadrenocorticism(PDH) related change.
Regarding the patient's blood work, the elevated liver enzymes may be due to possible hyperadrenocorticism. Specifically, the elevated GGT could be linked to PDH, primary hepatobiliary disease, or renal disease. Further work up for PDH was also recommended.
OUTCOME: The patient was asymptomatic and continues to do well. Three view thoracic radiographs were recommended to assess for metastatic lesions. The patient has been referred to a veterinary oncologist for further work up and therapy.
REFERENCES:
Cho SH, Seung BJ, Kim SH, Lim HY, Lee GS, Chae MS, Sur JH. Renal interstitial cell tumor in a dog: clinicopathologic, imaging, and histologic features. J Vet Diagn Invest. 2020 Jan;32(1):124-127. doi: 10.1177/1040638719897585. Epub 2019 Dec 26. PMID: 31876249; PMCID: PMC7003225.
Meuten DJ, Meuten TLK. Tumors of the urinary system. In: Meuten DJ, ed. Tumors in Domestic Animals. 5th ed. Raleigh, NC: Wiley, 2016:632–688
Melanie A. Breshears, Anthony W. Confer, Chapter 11 - The Urinary System1, Editor(s): James F. Zachary, Pathologic Basis of Veterinary Disease (Sixth Edition), Mosby,2017,Pages 617-681.e1,ISBN 9780323357753
Thank you to Shady Grove Animal Hospital and Eastern Vet Path for collaborating with us on this case.